New Zealand Primary care (Dunedin | Otago | Southland)
Sleeve gastrectomy (SG) is a laparoscopic bariatric procedure in which approximately 75–80% of the stomach (fundus and greater curvature) is resected, forming a narrow gastric tube (~100–150 mL capacity).
What should GPs monitor after gastric sleeve surgery?
After sleeve gastrectomy, New Zealand GPs should implement structured lifelong monitoring to prevent nutritional deficiency and detect surgical complications early. Patients typically achieve 30–35% total body weight loss (TBWL) at 12 months, with most weight reduction occurring in the first 6–8 months.
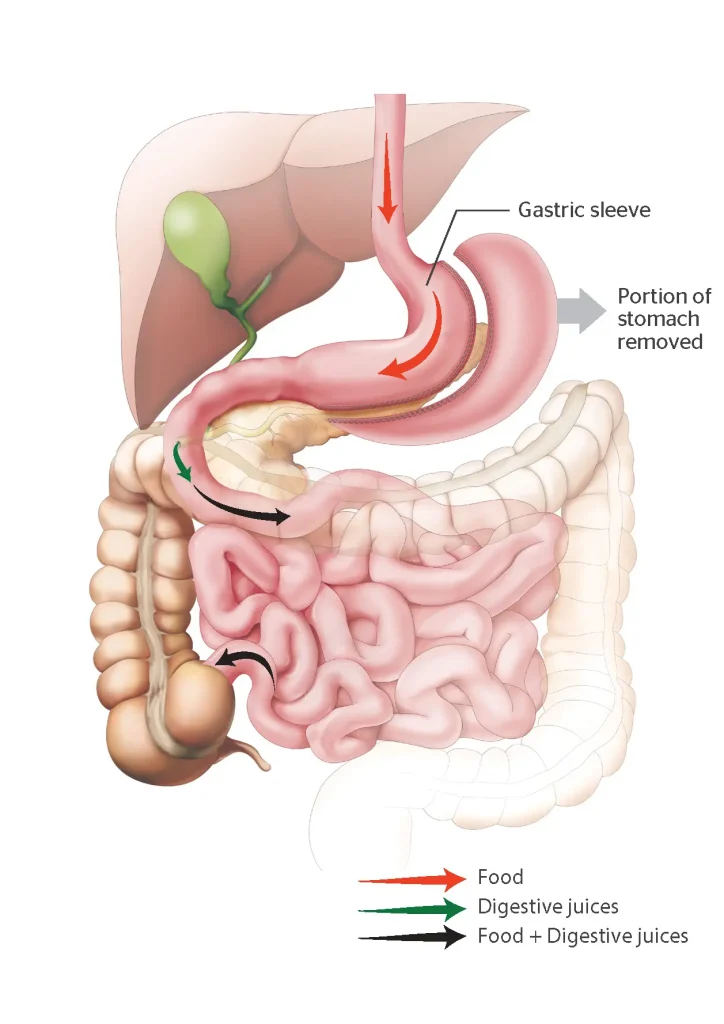
How does a Sleeve Gastrectomy work?
- Gastric restriction
- Reduced ghrelin production
- Improved satiety
- Enhanced insulin sensitivity
Unlike Roux-en-Y gastric bypass, SG does not involve intestinal bypass, but micronutrient deficiency remains a recognised long-term risk.
How much weight loss is expected after Gastric Sleeve surgery?
Weight loss is measured as % Total Body Weight Loss (TBWL).
- 1 month: 8–12% TBWL Rapid early phase
- 4 months: 18–25% TBWL Strong metabolic response
- 8 months: 25–32% TBWL Slowing trajectory
- 12 months: 30–35% TBWL Plateau common
Failure to achieve >10% TBWL by 6 months warrants dietary, behavioural and medical review.
Concerning Patterns
- <10% TBWL at 6 months
- Persistent vomiting
- Rapid unexplained weight loss
- Lack of metabolic improvement
Early and Late Complications
Early (<30 Days)
- Staple line leak
- Intra-abdominal collection
- Haemorrhage
- Pulmonary embolism
Late
- Gastro-oesophageal reflux
- Sleeve stricture
- Iron deficiency anaemia
- Vitamin B12 deficiency
- Gallstones
- Weight regain
What are the red flag symptoms to look for after a Sleeve Gastrectomy?
When should a GP refer urgently?
Urgent same-day referral required if:
- Tachycardia >100 bpm
- Severe abdominal pain
- Fever
- Shoulder tip pain
- Persistent vomiting
- Dysphagia
- Haematemesis or melaena
- Acute chest pain or dyspnoea
- Clinical dehydration
Tachycardia is often the earliest sign of a staple line leak.
If unstable in Otago/Southland → refer to Dunedin Hospital ED.
When to refer to the public hospital
- Suspected leak
- Ongoing obstruction
- Severe symptomatic anaemia (Hb <90 g/L)
- Intractable reflux
- Severe malnutrition
- Neurological B12 deficiency
- Symptomatic gallstones
Refractory reflux may require conversion to Roux-en-Y gastric bypass.
Recommended vitamin supplementation after a Sleeve Gastrectomy (NZ)
Are lifelong vitamins required after sleeve gastrectomy?
Yes. Despite being primarily restrictive, sleeve gastrectomy alters gastric physiology and intake patterns. Lifelong supplementation reduces risk of:
- Iron deficiency anaemia
- Vitamin B12 deficiency
- Vitamin D deficiency
- Secondary hyperparathyroidism
Although sleeve gastrectomy is restrictive rather than malabsorptive, long-term deficiency risk is well documented.
Core supplement regimen
- Bariatric-specific multivitamin (daily)
- Vitamin B12 (oral high dose or IM 3-monthly)
- Calcium citrate 1200–1500 mg/day
- Vitamin D 2000–3000 IU daily
- Iron (if menstruating or low ferritin)
Bariatric supplement providers in New Zealand
Bariatric-formulated products are preferred due to appropriate dosing of iron, B12, fat-soluble vitamins, and trace elements compared with standard pharmacy multivitamins.
Calcium citrate is preferred over carbonate due to improved absorption post-surgery.
What blood tests should GPs order after sleeve gastrectomy?
| Time Point | Tests to Request | Clinical Purpose |
| 1 Month | FBC, U&E, LFT, Iron studies, B12, Folate, Vitamin D | Assess hydration, early anaemia, baseline micronutrient status |
| 4 Months | FBC, Iron studies, B12, Folate, Vitamin D, HbA1c, Lipids, LFT | Monitor metabolic improvement and emerging deficiencies |
| 8 Months | FBC, Iron studies, B12, Folate, Vitamin D, Calcium, PTH, Albumin | Detect ferritin depletion, secondary hyperparathyroidism |
| 12 Months | FBC, Iron studies, B12, Folate, Vitamin D, Calcium, PTH, HbA1c, Lipids, Zinc, Copper (if indicated), Thiamine (if vomiting) | Comprehensive annual nutritional review |
| After 2 Years (Annually) | FBC, Iron studies, B12, Folate, Vitamin D, Calcium, PTH, HbA1c, Lipids | Lifelong surveillance to prevent late deficiency |
Increase frequency if:
- Ongoing PPI use
- Pregnancy
- Vegetarian/low-protein diet
- Heavy menstruation
- Poor oral intake
- Recurrent vomiting
How is reflux managed after Sleeve Gastrectomy?
Sleeve gastrectomy can worsen gastro-oesophageal reflux due to increased intragastric pressure.
Initial management: 8–12-week PPI trial.
Persistent severe reflux may require surgical reassessment and possible conversion to Roux-en-Y gastric bypass.
Management approach:
- PPI trial (8–12 weeks)
- Endoscopy if dysphagia
- Weight stabilisation
- Surgical review if refractory
Persistent severe reflux may require bariatric reassessment.
Medication review considerations
- Avoid NSAIDs where possible
- Review antihypertensives early
- Reduce insulin promptly post-op
- Avoid extended-release medications
Hypoglycaemia is common if diabetes medications are not adjusted early.
GP quick reference checklist
- Expect 30–35% TBWL at 12 months
- Lifelong bariatric multivitamin required
- Structured blood monitoring schedule
- Treat reflux early
- Urgent referral for tachycardia + abdominal pain
- Annual lifelong surveillance
This page is authored by Mark Grant, FRACS, Consultant Upper GI and Bariatric Surgeon, Dunedin. Southern Weight Loss provides specialist obesity care across Otago and Southland with integrated medical and surgical pathways.