Gastric Sleeve Surgery in Dunedin, Otago & Southland
Gastric sleeve surgery in Dunedin: key facts
Gastric sleeve surgery is a highly effective weight loss procedure that reduces stomach size and lowers hunger hormones. In New Zealand, it is typically offered to patients with a BMI ≥35, or ≥30 with related conditions such as type 2 diabetes or sleep apnoea. Most patients lose 60–70% of excess weight within 12–18 months. At Southern Weight Loss, surgery is performed in Dunedin with structured long-term follow-up across Otago and Southland.
What is gastric sleeve surgery?
Gastric sleeve surgery (sleeve gastrectomy) is a laparoscopic (keyhole) bariatric procedure designed to help patients achieve meaningful and sustained weight loss.
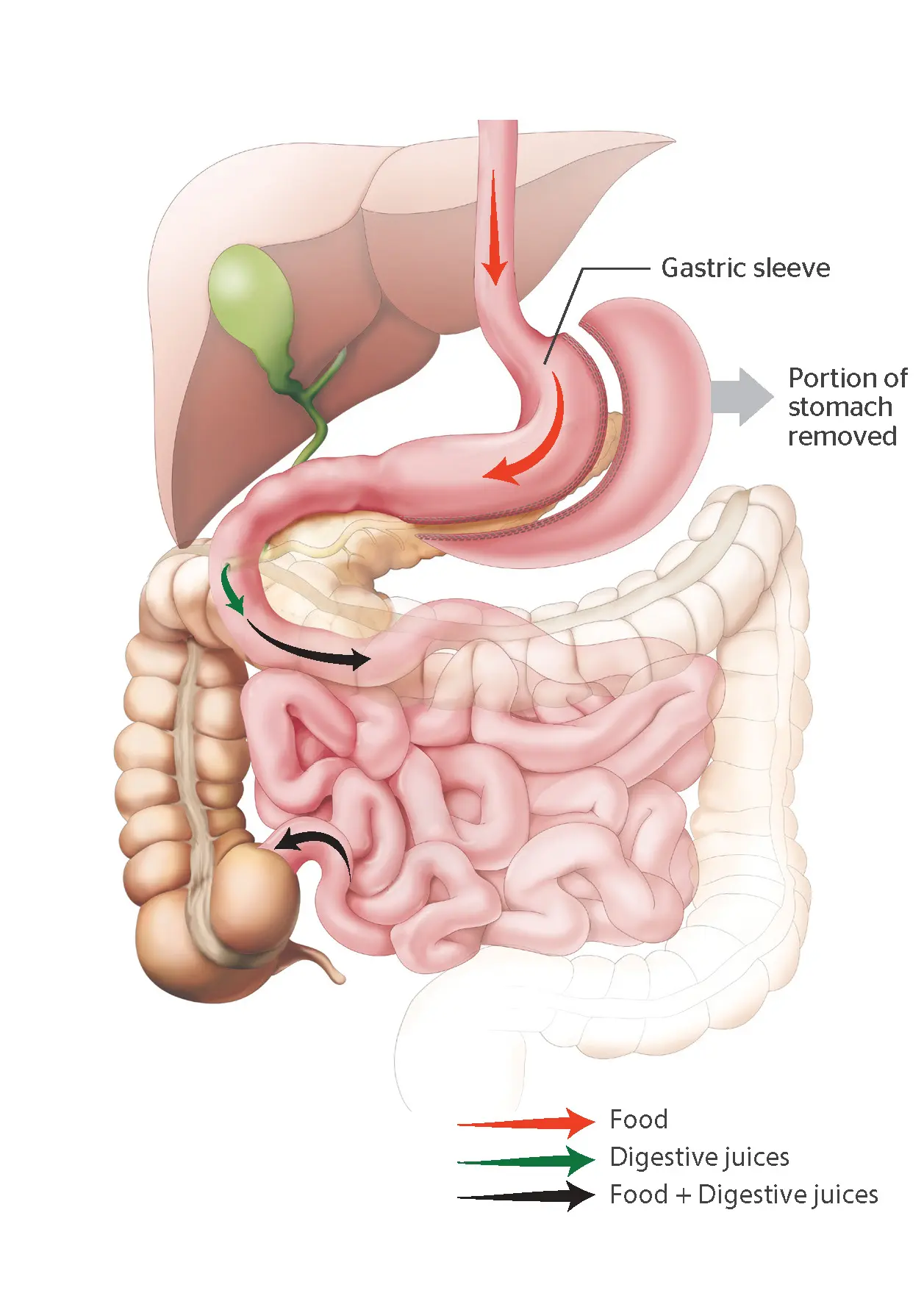
During the operation, approximately 75–85% of the stomach is removed, leaving a narrow tube or “sleeve.” This significantly reduces the volume of food that can be eaten and alters how the body regulates hunger and fullness.
Unlike gastric bypass, the digestive tract is not rerouted. Food continues to pass through the stomach and intestines in a normal sequence, which simplifies the anatomy while still delivering strong metabolic effects.
How does gastric sleeve surgery work?
Gastric sleeve surgery works by reducing stomach size and lowering levels of ghrelin, the hormone that drives hunger. The smaller stomach limits food intake, while hormonal changes reduce appetite and improve satiety. These combined effects help patients eat less, feel satisfied earlier, and maintain weight loss over time.
Importantly, this is not just a mechanical restriction.
Patients often experience:
- Reduced background hunger
- Fewer intrusive food thoughts (“food noise“)
- Improved control over eating behaviours
This shift is one of the key reasons gastric sleeve can be effective where repeated dieting has failed.
The biology behind weight regain
Many patients considering surgery have experienced cycles of weight loss and regain.
This is not simply about willpower.
When weight is lost:
- Hunger hormones increase
- Metabolism slows
- The brain increases focus on food
This creates a strong biological drive to regain weight.
Gastric sleeve helps counter these effects by:
- Reducing hunger signals
- Improving satiety
- Supporting a more sustainable weight “set point”
Who is gastric sleeve suitable for?
Indications
Gastric sleeve may be appropriate if you:
- Have a BMI ≥35, or ≥30 with weight-related conditions
- Have struggled with long-term weight regain
- Have tried structured diet, exercise, or medications without lasting success
- Prefer a simpler surgical option without intestinal bypass
- Are earlier in your weight loss journey
It is commonly used:
- As a first surgical option
- In patients without severe reflux
- In those seeking a balance between effectiveness and complexity
Who is eligible for gastric sleeve in New Zealand?
Gastric sleeve surgery is typically offered to patients with a BMI ≥35, or ≥30 with obesity-related conditions such as diabetes, high blood pressure, or sleep apnoea. It is often suitable for patients seeking a simpler surgical option or those earlier in their treatment journey. A full specialist assessment is required to determine the safest and most appropriate treatment.
Eligibility also considers:
- Medical history
- Previous abdominal surgery
- Eating behaviours
- Long-term goals
Gastric sleeve vs other weight loss treatments
Choosing the right treatment is one of the most important decisions in your journey.
Is gastric sleeve better than bypass or medications?
Gastric sleeve surgery provides significant weight loss with a simpler anatomical approach than gastric bypass. It is often preferred for patients without severe reflux or advanced metabolic disease. Medications such as GLP-1 therapies can support weight loss, but typically require ongoing use. The best option depends on individual health, goals, and long-term planning.
Comparison of treatment options
| Treatment | Expected weight loss | Best for | Considerations |
|---|---|---|---|
| Gastric sleeve | 60–70% excess weight | Simpler surgery, early intervention | May worsen reflux |
| Gastric bypass | 65–80% | Diabetes, reflux, revision | More complex, lifelong supplements |
| GLP-1 medications | 10–20% total body weight | Non-surgical option | Requires ongoing treatment |
How gastric sleeve surgery is performed
Procedure
Gastric sleeve surgery is performed laparoscopically under general anaesthetic.
The operation involves:
- Removing a large portion of the stomach
- Creating a narrow sleeve-shaped stomach
- Sealing the stomach with a staple line
The remaining stomach typically holds 80–120 mL, significantly reducing food intake.
What happens during surgery?
- Small incisions are made in the abdomen
- A camera and surgical instruments are inserted
- The stomach is divided using stapling devices
- The removed portion is extracted
The operation usually takes:
- 1–2 hours
- Hospital stay: 1–2 nights
Benefits of gastric sleeve surgery
Benefits
Gastric sleeve offers a strong balance between effectiveness and simplicity.
How much weight can you lose after gastric sleeve?
Most patients lose approximately 60–70% of their excess body weight within 12–18 months after gastric sleeve surgery. Weight loss is typically most rapid in the first 6–9 months before stabilising. Long-term success depends on nutrition, activity, and structured follow-up support.
Metabolic improvements
- Improved blood sugar control
- Reduced insulin resistance
- Lower blood pressure
- Improved cholesterol levels
Some patients:
- Reduce medications
- Improve or resolve type 2 diabetes
Quality of life improvements
- Increased energy
- Improved mobility
- Reduced joint pain
- Better sleep
Behavioural changes
Patients often report:
- Feeling full sooner
- Reduced cravings
- Improved ability to follow structured eating
Risks and complications
Complications
All surgery carries risks, and these are discussed in detail during consultation.
What are the risks of gastric sleeve surgery?
Gastric sleeve surgery is generally safe, but complications can occur. Early risks include bleeding, infection, or leaks from the staple line. Longer-term risks may include reflux, nutritional deficiencies, or weight regain. Careful surgical technique and structured follow-up help minimise these risks and support long-term success.
Early risks
- Bleeding
- Infection
- Staple line leak
- Blood clots
Longer-term risks
- Reflux (GORD)
- Sleeve stenosis (narrowing)
- Nutritional deficiencies
- Weight regain
What to expect after gastric sleeve surgery
How long does it take to recover from gastric sleeve?
Most patients stay in hospital for 1–2 days and return to light activities within 1–2 weeks. Full recovery typically takes 4–6 weeks. Patients follow a staged diet progression and gradually increase activity, supported by regular follow-up to optimise long-term outcomes.
Early recovery (weeks 1–4)
Focus on:
- Hydration
- Protein intake
- Healing
Diet stages:
- Fluids
- Purée
- Soft foods
Medium-term recovery (1–6 months)
- Continued weight loss
- Increasing activity
- Expanding diet
Long-term phase
Success depends on:
- Consistent eating patterns
- Protein prioritisation
- Strength training to maintain muscle
- Ongoing follow-up
Life after gastric sleeve
Gastric sleeve is a tool that works best with support.
Patients who succeed long-term:
- Maintain structure in eating
- Understand hunger vs cravings
- Stay connected to follow-up care
Why weight loss slows over time
Weight loss typically:
- Rapid early phase (first 6–9 months)
- Slower phase after
This is normal and reflects:
- Metabolic adaptation
- Body reaching a new equilibrium
Preventing weight regain
Key strategies:
- Regular follow-up
- Adequate protein intake
- Strength training
- Early identification of challenges
Why choose Southern Weight Loss?
Your surgeon: experience matters in bariatric surgery
Choosing to undergo gastric sleeve surgery is a significant decision, and outcomes are influenced not only by the procedure itself, but by the experience of the surgeon and the structure of care around you.
At Southern Weight Loss, surgery is performed by Mark Grant, an Upper Gastrointestinal and Bariatric Surgeon based in Dunedin.
Mark Grant is a Fellow of the Royal Australasian College of Surgeons (FRACS), with specialist training in bariatric and oesophagogastric surgery in both New Zealand and the United Kingdom. He completed advanced fellowship training at University Hospital Southampton and returned to New Zealand to undertake dedicated bariatric training at Waitematā DHB.
His practice focuses on:
- Gastric sleeve surgery
- Gastric bypass surgery
- Revisional bariatric procedures
- Management of reflux and upper GI conditions
This combination of experience is important, particularly when:
- Selecting the most appropriate procedure
- Managing complications if they arise
- Supporting long-term outcomes
A multidisciplinary approach to long-term success
One of the key differences in bariatric outcomes is not just the operation—but the structure of care after it.
At Southern Weight Loss, care is delivered through a coordinated multidisciplinary team, including:
- Surgeon
- Dietitian
- Psychological support
This team works together to:
- Prepare patients before surgery
- Support recovery after surgery
- Identify challenges early
- Maintain long-term results
This approach reflects modern understanding that obesity is a chronic condition requiring ongoing management, rather than a single intervention.
Why local care changes outcomes
Patients across Otago and Southland often face a choice between:
- Local care with ongoing support
- Visiting or remote surgical providers
There are important differences.
Mark Grant provides care locally in Dunedin, with follow-up available across Otago and Southland. This allows patients to access specialist treatment and ongoing support without needing to travel out of the region.
Local care supports:
- Easier access to follow-up appointments
- Faster response to complications or concerns
- Better continuity of care
- Stronger long-term engagement
These factors are closely linked to:
- Reduced complication rates
- Better weight maintenance
- Improved patient experience
Experience with the full spectrum of bariatric care
At Southern Weight Loss, patients are assessed across:
- Gastric sleeve
- Gastric bypass
- Revisional surgery
- Medical weight loss options
Bariatric surgery is most effective when treatment is tailored to the individual, rather than applying a one-size-fits-all approach.
Continuity from first consultation to long-term follow-up
Patients are typically seen:
- Before surgery
- At regular intervals after surgery
- Long-term as needed
This continuity allows:
- Monitoring of nutrition
- Adjustment of treatment plans
- Early identification of weight regain
- Ongoing support for behaviour change
This is particularly important because:
- Weight loss slows over time
- Biological drivers of weight regain persist
- Long-term success depends on sustained support
Where is gastric sleeve surgery performed in Dunedin?
Gastric sleeve surgery at Southern Weight Loss is performed locally in Dunedin by an experienced bariatric surgeon, with follow-up care across Otago, Queenstown and Southland. Patients benefit from a consistent local team and structured long-term support, rather than a visiting or remote model of care.
Frequently asked questions
How much weight can I lose?
Most patients lose 60–70% of excess weight within 12–18 months.
Is gastric sleeve permanent?
Yes. The removed portion of the stomach cannot be reversed.
Will I feel less hungry?
Yes—many patients experience reduced hunger due to hormonal changes.
Can weight regain happen?
Yes. Long-term success depends on ongoing habits and support.
What happens if sleeve doesn't work?
Conversion to gastric bypass may be considered in selected cases.
Start your journey
If you are considering gastric sleeve surgery in Dunedin, Otago, or Southland, the first step is a consultation.
Southern Weight Loss provides:
- Expert assessment
- Personalised treatment planning
- Long-term local support
Self-referrals welcome